Please use this identifier to cite or link to this item:
http://hdl.handle.net/20.500.12188/27686| DC Field | Value | Language |
|---|---|---|
| dc.contributor.author | C. Volkanovska Ilijevska | en_US |
| dc.contributor.author | M. Zivkovic Hristova | en_US |
| dc.contributor.author | M. Dimitrovska | en_US |
| dc.contributor.author | S. Jovanovska Mishevska | en_US |
| dc.date.accessioned | 2023-09-04T11:05:26Z | - |
| dc.date.available | 2023-09-04T11:05:26Z | - |
| dc.date.issued | 2022-10-13 | - |
| dc.identifier.uri | http://hdl.handle.net/20.500.12188/27686 | - |
| dc.description.abstract | Hyperthyroidism raises the risk of maternal and fetal complications. Hence early detection and treatment of hyperthyroidism in a pregnancy is imperative. Management of Graves' hyperthyroidism in pregnancy remains a challenge for physicians. The transplacental passage of maternal thyroid stimulating antibodies (TSHrAb) and antithyroid drugs (ATD) could have detrimental effect on fetal development. Additionally, maintaining sufficient thyroid hormone levels in maternal circulation during the treatment with ATD is essential, as thyroid hormones are crucial factors for normal development of the fetus, particularly the fetal brain. Additionally, ATD must be carefully titrated in order to avoid fetal hyper-or hypothyroidism. One more concern of use of ATD in pregnancy is the potential risk for severe birth malformations when fetus is exposed to ATDs in 6 to 10th gestational week(gw) of pregnancy. We present a pregnant woman at 6th gw with uncontrolled hyperthyroidism. Thyroxine and triiodothyronine values were four times above reference values, TSH was significantly suppressed and TSHrAb were 10fold increased. Ultrasound measurement of thyroid volume was >50ml. The patient was treated with maximum recommended doses At25 gw the TSHrAb significantly decreased and a careful reduction of ATD to a minimum maintenance dose was achieved during the period 26 to 34gw. The outcome and course of the pregnancy was uneventful. Due to delicate balance of benefit and potential risk of use of ATD for optimal fetal development and fetal thyroid function management of hyperthyroidism in pregnancy requires teamwork between gynecologist and an endocrinologist. | en_US |
| dc.language.iso | en | en_US |
| dc.subject | hyperthyroidism | en_US |
| dc.subject | pregnancy | en_US |
| dc.subject | ATD | en_US |
| dc.title | CASE REPORT: MANAGEMENT OF GRAVES DISEASE DURING PREGNANCY | en_US |
| dc.type | Proceeding article | en_US |
| dc.relation.conference | 6th Macedonian Congress of Endocrinology | en_US |
| item.fulltext | With Fulltext | - |
| item.grantfulltext | open | - |
| crisitem.author.dept | Faculty of Medicine | - |
| Appears in Collections: | Faculty of Medicine: Conference papers | |
Files in This Item:
| File | Description | Size | Format | |
|---|---|---|---|---|
| Graves.png | 82.35 kB | image/png | 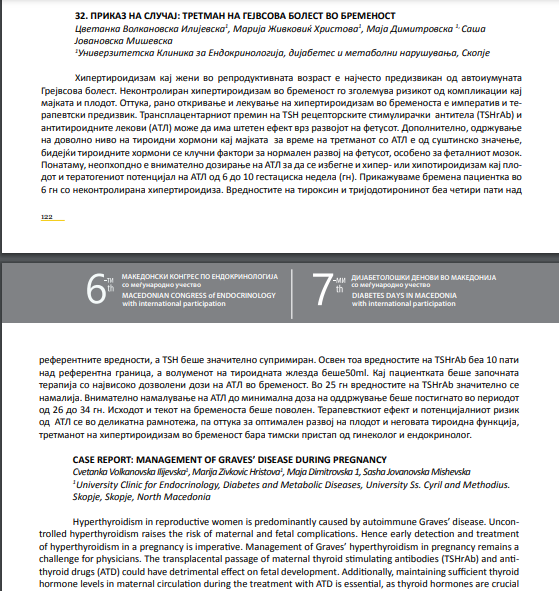 View/Open | |
| Насловна.png | 240.43 kB | image/png |  View/Open |

Items in DSpace are protected by copyright, with all rights reserved, unless otherwise indicated.